
You Are Not The Average
Embracing Individual Differences Could Transform How We Evaluate Evidence


ENERGY SCIENCE
Decades of research have been invested in an effort to better understand what we can do to live healthier, longer, and fuller lives. However, one thing that is consistent across nearly all studies on human health is that different people respond differently to most treatments.
Peel the surface of any clinical trial and you’ll see one striking thing: nobody is the average.
Each person is truly unique
One area where this principle shines clearly is diet and nutrition.
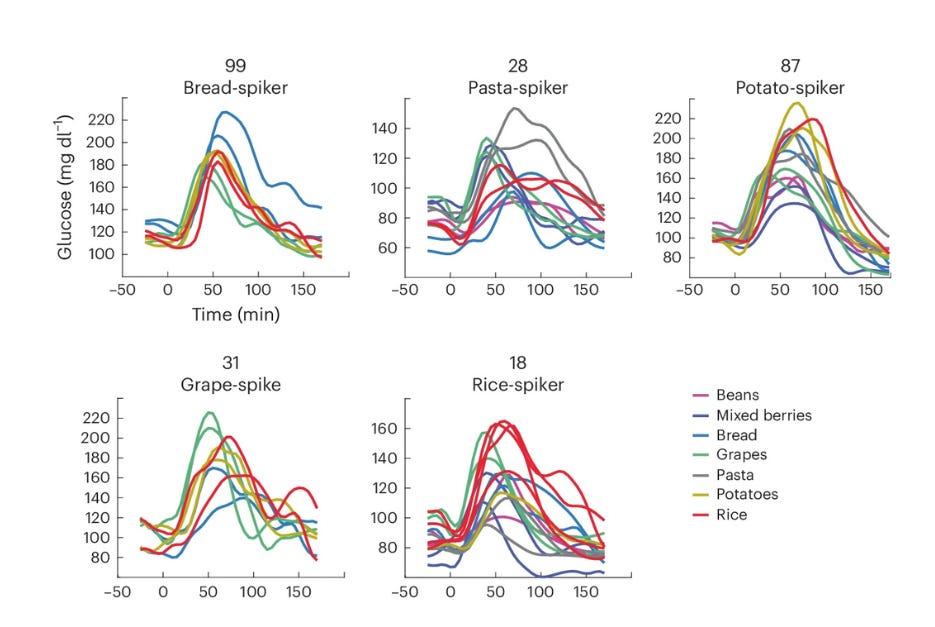
The ways the human body responds to diet, and how individuals feel after eating particular foods, are highly individual. Everyone is unique, and everyone’s body responds to food slightly differently.
Why don’t all human beings have the same tastes? Why do individuals prefer some foods over others?
When it comes to making decisions about your diet and nutrition, the most relevant questions for you are: what foods fuel your body and your brain to operate optimally? And what foods make you feel your best?
The way we’ve been doing science all these years hasn’t equipped us to answer these questions. And this impacts our health and well-being.
The Classic Clinical Trial
In his recent article on ultra-processed foods, David S. Ludwig emphasizes, like other academic medical scientists have for decades, the need for ‘clinical trials.’ In particular, he recommends conducting long-term clinical trials of different diets that extend beyond just a few weeks or months.
On the surface, this seems like a reasonable call to action. But what is a clinical trial? How do they give us the truth—or rather, what kind of truth do they yield?
In randomized controlled trials (RCTs), you first establish the most critical or valuable outcome. Perhaps you want to know if Diet A or B can change a person’s disease symptoms. Your outcome could also be a subjective human experience like fatigue or depression, for example. Or it could be something you can objectively measure in the blood like inflammation or insulin. For now, let’s stick with depression.
Once you’ve identified what you want to change—say, depression symptoms—then you recruit dozens to hundreds of people. The more people, the more statistical power you have. This means that with more people in your study, you increase the probability of finding an effect if there is one, and you reduce the probability of missing a real effect.
Once you’ve recruited your sample (a subgroup of the population you aim to understand), you randomize people into two or more groups: Diet A and Diet B, for example. You measure their baseline mental health status before making any changes to their diet.
Then you deploy the intervention or treatment. You wait while participants in the study complete the protocol for the group they were assigned. And when the wait is over, you measure their depressive symptoms again.
Once you know the change in depression for individuals in both groups, you lump all participants in the Diet A group together and calculate an average. You repeat this for everyone in the Diet B group and get the average. And then comes the moment of truth.
You compare the group average changes in symptoms.
Essentially, the purpose of a standard RCT is to determine if a treatment differently and significantly change the primary outcome—on average.
So, on average, did the participants on Diet A become significantly less depressed than the participants on Diet B?
The Limitations of Comparing Averages
When we perform a clinical comparing Diet A and Diet B, we’re not comparing the responses of individual participants. We’re comparing the average of all the participants in the Diet A group to the average of all the participants in the Diet B group.
The scientific rationale is as follows: by prioritizing average effects over individual changes, you avoid ‘noise’ and find out what is generally true. It smooths the signal and flattens the variability in the data.
But my point is this: our science of averages is hurting (at least some of) us.
We study averages for pragmatic reasons. We rely and value large sample size studies over small ones because they offer more statistical power. And we view n-of-1 case reports with skepticism (or often with dismissal) because they don’t represent everyone.
But the average doesn’t represent anyone.
You are not the average. I am not the average. Nobody actually is the average.
There are good reasons to be skeptical about single person observations, but there are great consequences too. The structure of our science is set up so that we value average changes over individual effects, even if those individual effects are curative, life-changing, and personally meaningful.
Unlike what the medical textbooks state, what our average-based science reports, and what clinical trials assume, everyone’s body works a little differently. That’s the whole premise behind personalized medicine. It’s true.
Everyone is somewhat unique. And a drug that works for one person may not work for another. But a trial of averages has no way of detecting this.
How a Science of Averages Impacts Health
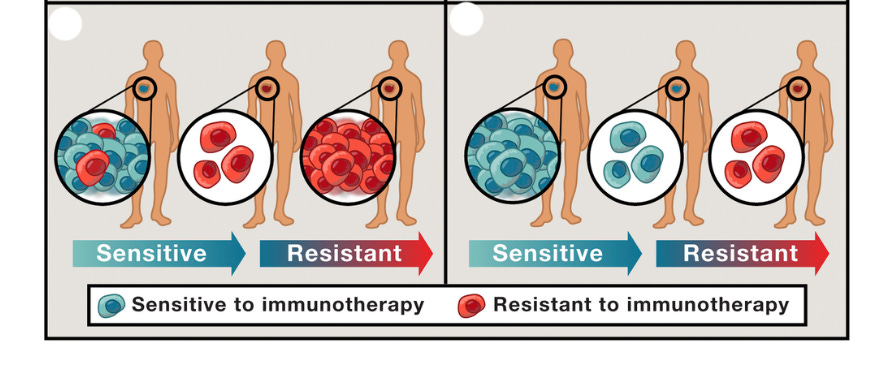
There could already be cancer treatments out there that each work wonders on 5-20% of the population. Effective treatments that cure a small portion of people.
For example, there could be effective cures for schizophrenia, bipolar disorder, or other mental illnesses out there—treatments that put lifelong diagnoses into permanent remission in 10-20% of affected people.
And there could be different anti-aging strategies that truly add 1-2 decades of healthspan to some people’s lives.
And we’ll never know.
If we rely on RCTs alone—we’ll never know, and therefore we’ll never use them. That’s because, although they may work seemingly miraculously on some people, once you lump these people with hundreds of others whose bodies and minds work differently (and who don’t respond to that one treatment), group statistics obscure that truth.
For instance, only 20-40% of cancer patients respond to immunotherapy.
In studies of averages, the real, precious, important individual signal gets drowned in a mythical average that represents no one.
If the RCT “fails,” the potential treatment is deemed “ineffective”—for everyone. And so it gets lost.
When an RCT fails, the gold standard clinical trial has spoken. Diet, treatment, or intervention A is (on average) not any better than B. Case closed–even if it saved a few lives.
That average-based knowledge, then, becomes like a pernicious fluid that floods science. “Yeah, but the clinical trial failed—there is no effect (on average).”
What if the patient sitting there in front of you is part of that 5% or 20% who would have benefitted?
The Value of Incorporating Individual Experiences
There are things people know empirically (which means ‘from experience’) to be true. They know how they feel when they eat something. Or when they do a certain activity. Or they might know this drug or treatment is hurting them.
Yet when they talk to a well-meaning scientist or to their doctor, they may be told they’re wrong because of some clinical trial showing that (on average) people don’t respond the way they seem to.
This is something I discussed in my recent interview with Andrew Huberman on his Huberman Lab Podcast.
By focusing on and upholding our science of averages above human experiences, we do ourselves a disservice. We propagate average truths that apply to only a portion of people, squashing meaningful, potentially life-changing, and health-promoting information for many.
As Dr. Ludwig pointed out, it’s possible that eating a lot of fat is bad for some people (a dogma propagated by a dubious commercial-academic partnership in the 1960’s), but we don’t have good data to show this.
In fact, biologically, if you feed cells in a dish lots of fat (no sugar), they make more mitochondria—a process called mitochondrial biogenesis. If you don’t feed them fat and give them sugar only, they get rid of a lot of their mitochondria.
Some people go on fat- and protein-only diets—called the ketogenic diet—and feel fantastic. Some have seen their diabetes reverse, their neurodegenerative disease slow down or even reverse, their tumor shrinks, or their psychotic symptoms of schizophrenia vanish.
These people may be the 5-20%, or there may be many more like them. They deserve to be understood for their own sake, but also because others may have been dissuaded from pursuing those treatment options because of ‘average’ clinical trial results.
On the other hand, we know from clinical and personal experiences that eating too many carbohydrates can seriously hurt some people’s health. Clinical trials also support this. Do carbs hurt everyone? Probably not. You? Perhaps you’re one of those highly vulnerable ones. Or perhaps you’re not. Maybe we intuitively know the things that are good or not so good for us.
But a traditional clinical trial won’t give us the answers to these questions. So what will? We’re still working on figuring that out.
A Case in Point for Clinical Trial Reform
Clinical trials have helped us make some very important advances in medicine, and they have been instrumental in assessing the safety of drugs that are marketed to the public.
However, they are now—blindly perhaps—regarded as the gold standard in biomedicine.
Clinical trials guard us against the lure of unreproducible claims and anecdotes. If you’re going to develop a drug or other treatment for the mass market, you want it to work on a “majority” of people. It doesn’t need to work on everyone.
Clinical trials allow profitable drugs to be tested and approved. Their goal isn’t to find out the full truth about how certain diets affect the health of each person, nor what foods are the right foods for each individual. We need a finer-grained approach that considers individuality.
Do we need clinical trials to determine if ultra-processed foods are bad for the health of our developing children and the population at large? Maybe not.
Hypothetically speaking, what if ultra-processed foods were damaging the health of one out of every four (25%) children and adults? And what if ultra-processed foods that are easier to digest were health-promoting for those who have highly active lifestyles? Maybe because the chemical simplicity relieves the digestive system of the extra work of digesting whole foods.
Would we ever be able to find out things like this in a clinical trial?
We wouldn’t. After a couple years of following hundreds or thousands of kids and adults, we would get a typical answer from the trial. Maybe the researchers would report something along these lines:
“this prospective trial reveals that, after controlling for (some) confounders, ultra-processed foods had a negligible effect on metabolic health, cognitive function, and well-being.”
If we peeled off the layer of the trial’s average cover, we would likely find kids who did terrific and improved on several metrics. Some kids would likely exhibit no change, remaining close to the average. And some kids would show profound deterioration on one or more metrics. Are ultra-processed foods bad? On average, maybe so, maybe not. For some people, yes; and for others, no.
The Future of Clinical Trials for Enhancing Health
As a scientist in behavioral medicine, I worry that by continuing to regard clinical trials (as they are currently conducted) above all else, we won’t find the answers we are really looking for to improve our health.
We’re still using a tool designed decades ago to help standardize and regulate the mass marketing of drugs to get insights into highly personalized, individualized answers about our health.
It’s time for science to embrace individuality.
Having learned that the source of our differences is not in our genome, we need to think of new approaches to combine scientific rigor with the immense and irreplaceable value of human experiences.
But what does that look like in the context of researching diet and other interventions and therapeutics to optimize our health?
Maybe we need to incorporate first-principles thinking.
For example, to get a better understanding of our ideal individualized diet, perhaps we need to think about what kinds of foods we evolved to eat. Over hundreds of thousands of years, what foods fed the bodies of our ancestors? Think of your grandparents, and their parents, and keep going for a few thousand generations. The food they ate is what fueled the biological lineage you came from. What did your biology evolve from?
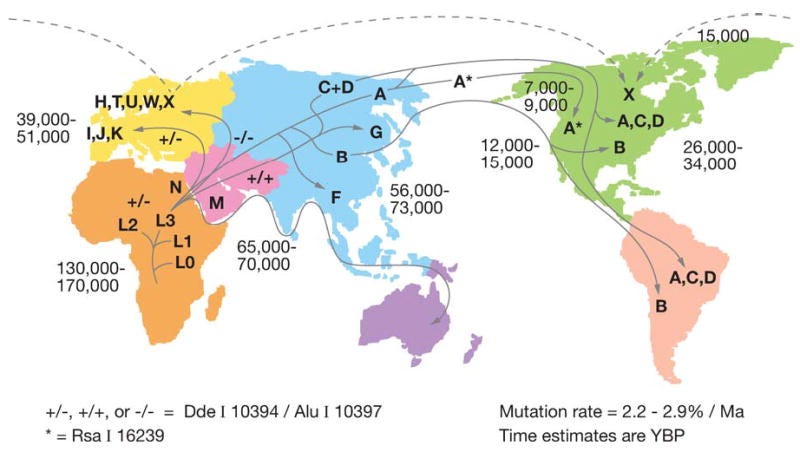
Perhaps region-specific whole foods are part of the answer. We all have different mitochondria based on where our ancestors came from.
Beyond thinking about the evolutionary or genetic contributions, there are a myriad of other factors and interactions to consider. These include our everyday environments, physical activity, stress, gut microbiome, inflammation, and yes, even the efficiency of your mitochondria in converting food into fuel.
Developing larger, more comprehensive datasets that consider a whole person within the context of their everyday life, such as the MiSBIE study, may help us get closer to truly understanding what we can do to optimize health for each individual person.
Moving Forward
People are complex. The research and medical communities need to push beyond the comfortable science of averages that we have grown accustomed to. With an aging population and many chronic diseases on the rise, despite substantial medical advances, this is more important now than ever before.
We need to work together to create new frameworks and approaches to capture and interpret individual differences to move us towards a model of fully personalized medicine that will best serve each of us.
You are not the average. Perhaps we need to cultivate the self-awareness that can guide each of us to adopt the behaviors and habits that are best suited for us—each a unique individual.
You and your ability to feel are the most sensitive instruments to know whether what you do, what you eat, and the content of your life is aligned with who you are as a person.
As the ENERGY book will discuss (sorry it’s taking so long to write!), integrating our ability to tune in to our experience together with scientific principles and data to guide our daily decisions may be the best way forward for each of us to flourish and fulfill our potential.
Curious how health emerges from the interplay between our biology and experience? Explore Columbia University’s Science of Health Program.
I love this. It’s the biological realization of what Boltzmann taught about statistical mechanics: the average tells you everything about the population, but nothing about the particle.
I’ve been working on a similar thread—looking at metabolism not as a set of fixed ranges, but as a Boltzmann-style distribution of energy and flow. Different entry point, but I think we are describing the same fundamental principle from two different sides of the aisle.
https://substack.com/home/post/p-190148509
I can’t disagree with anything you wrote. I am not even sure if I can add anything else. Clinical trials are important but limited. People are complex and when we add, different gut bacteria ( you already said), genetics, mitochondrial efficiency ( you said), evolutional impact (you wrote -for example hunter gatherer based ancestry ie the University of Bologna finding of longevity in higher Western Hunter Gatherer genes population in Italy). So, you are right. Add in, state of inflammation, mutations in cytokines, like interferon, age , exposure to light, indoor living under LEDs, underlying disease ( Lyme disease example). Kidney disease, environmental toxins, etc.